
LESSON 12 – Atrial Fibrillation (AF)
Arrhythmia substrate: In atrial fibrillation (AF), cardiac rhythm is not governed by a single sinus node but by multiple, chaotic ectopic foci arising simultaneously throughout the atria. As a result, coordinated atrial systole is absent, and normal P waves are not observed. Instead, the ECG demonstrates so-called f waves, which will be discussed further below.
Atrioventricular (AV) nodal conduction remains intact; therefore, ventricular activation occurs via the normal conduction system. However, due to the irregular arrival of impulses at the AV node, ventricular response becomes irregular, resulting in variability of the RR intervals. Additionally, impulses reach the ventricles at different phases of refractoriness, which may affect the amplitude of the R waves, leading to their alternation.
Based on this pathophysiological mechanism, the principal ECG features of Atrial Fibrillation can be summarized as follows:
- Absence of P waves.
- Presence of chaotic f waves instead of P waves (best visualized in leads II and V1). Note that these waves may not always be clearly distinguishable and can resemble baseline wander.
- Irregular RR intervals.
- Variation in R-wave amplitude (R-wave alternans), a non-specific and non-constant finding.
Clinical note: The presence of an irregular ventricular rate in combination with a non-sinus rhythm should prompt consideration of atrial fibrillation. AF is one of the most common arrhythmias, particularly in older individuals.
Let us consider several ECG examples of atrial fibrillation.
ECG Example 1 – Atrial Fibrillation
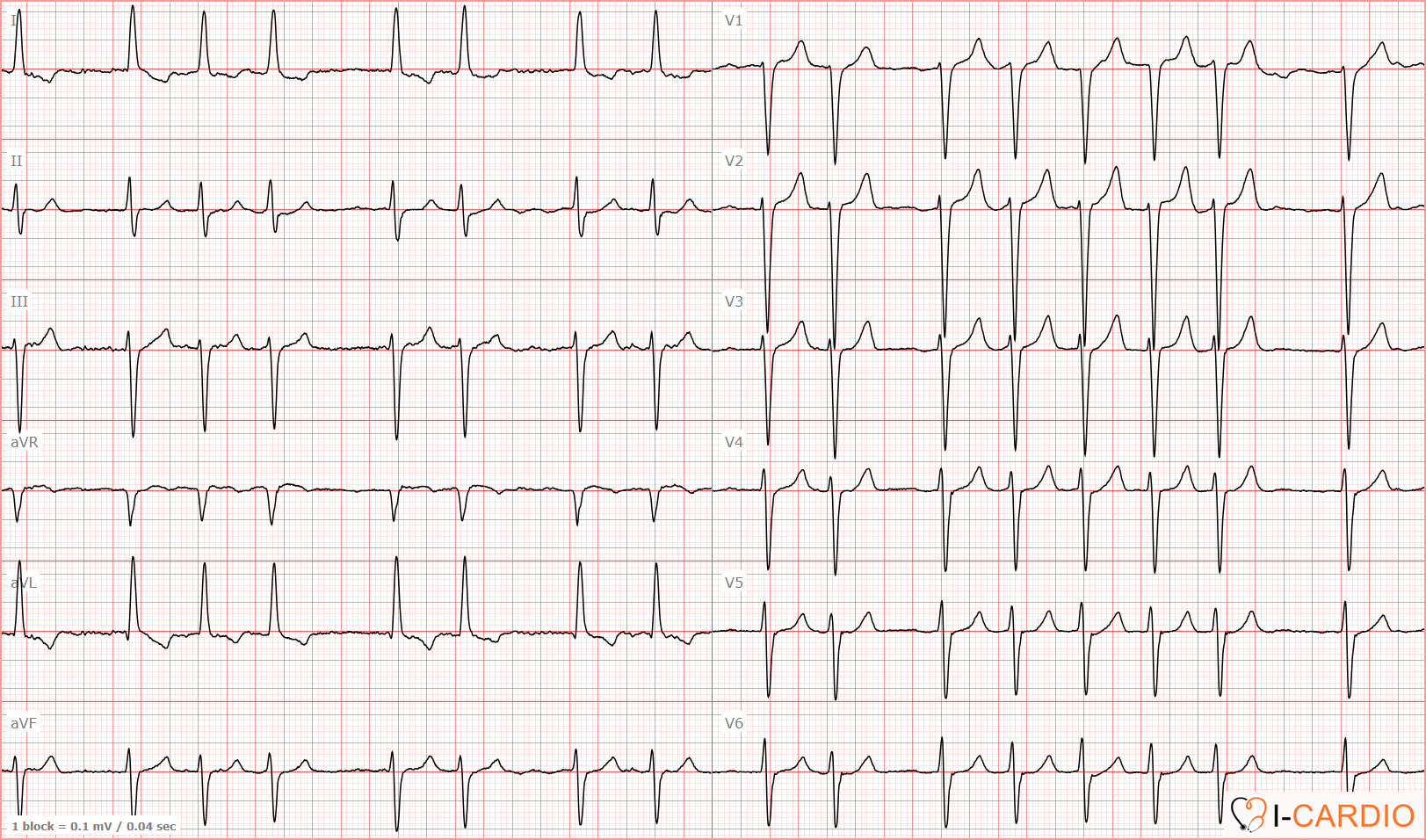
This ECG demonstrates an irregular tachycardia with no discernible P waves in leads II, V1, or V2.
Notably, prominent f waves (as frequently illustrated in textbooks) are not observed. However, clear R-wave alternans is present.
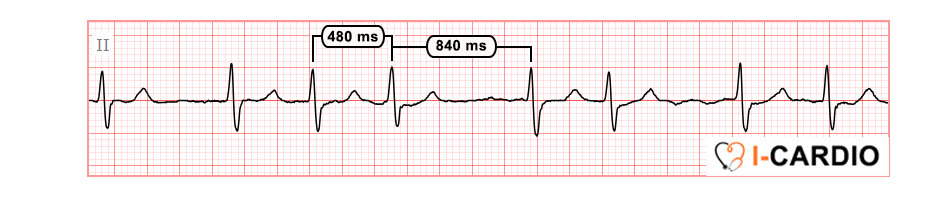
ECG Example 2 – Atrial Fibrillation

This ECG demonstrates an irregular tachycardia with a heart rate of up to 176 bpm, without discernible P waves in leads II, V1, or V2. Prominent f waves are present, as well as distinct R-wave alternans.

Atrial fibrillation is not invariably accompanied by tachycardia. Under the influence of chronotropic (rate-controlling) agents, the ventricular response may be within the normal range or even bradycardic.
ECG Example 3 – Atrial Fibrillation
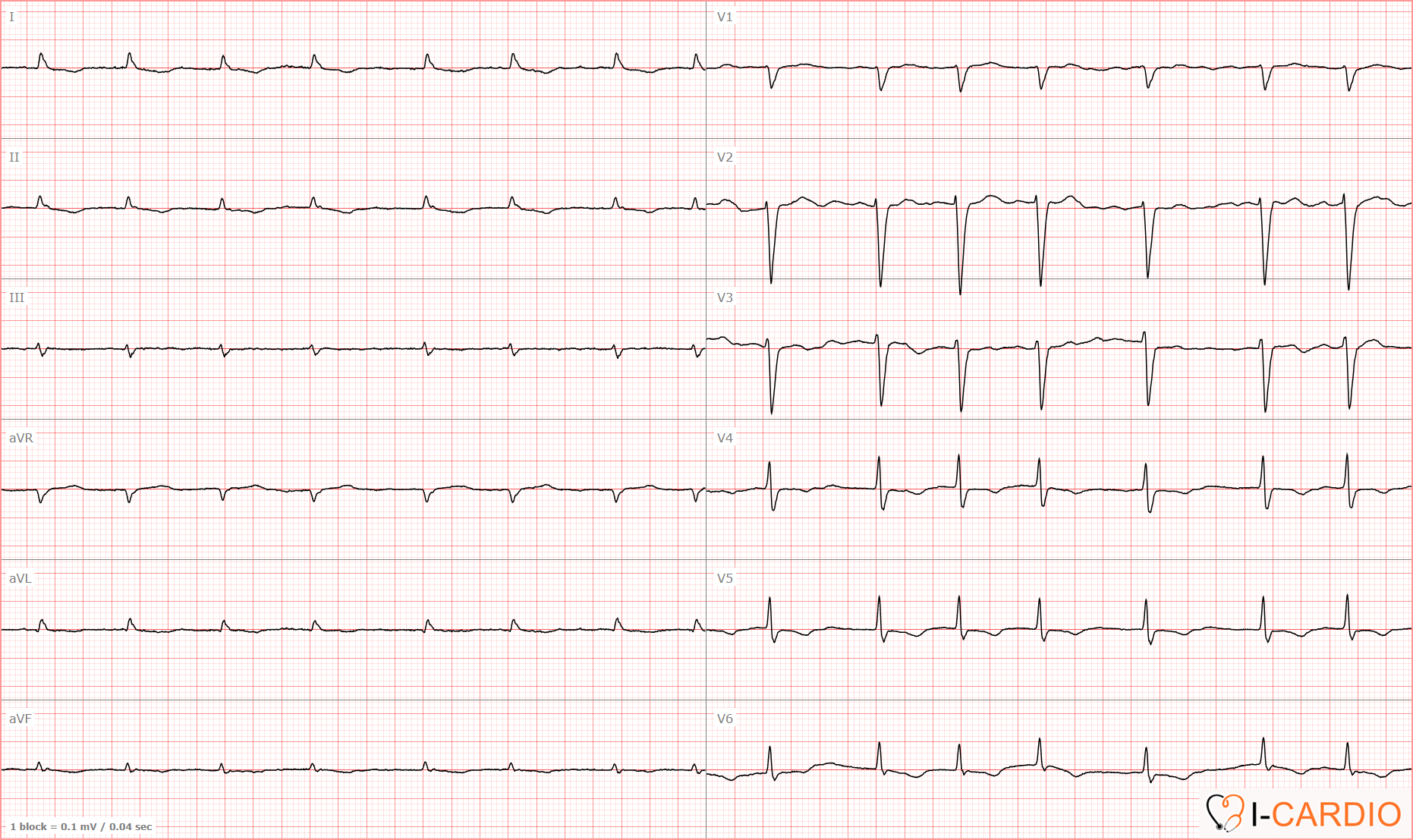
The heart rate, calculated from the first 5 RR intervals, is approximately 90 bpm.
All ECG criteria of atrial fibrillation are present: the rhythm is irregular, with variability of approximately 23%; there are no clearly identifiable P waves in leads II, V1, or V2.
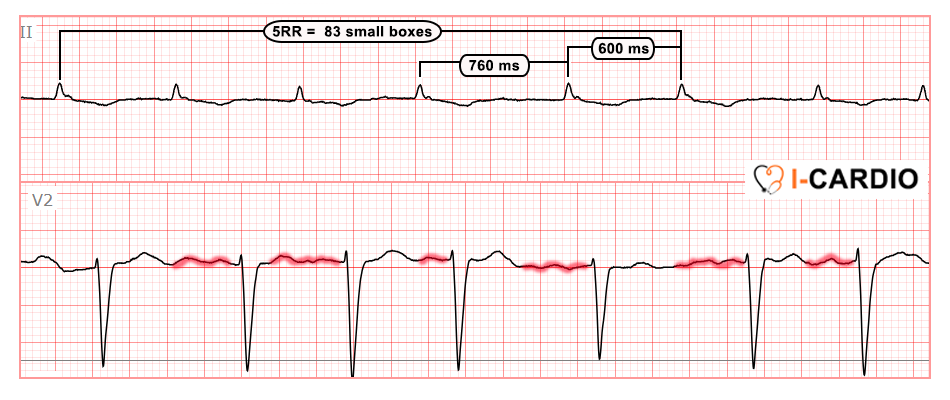
At the same time, fairly prominent f waves are present, along with a clear alternation in R or S-wave amplitude – this finding is most clearly observed in lead V2.
“There is one important exception in which the ventricular rate may appear regular in atrial fibrillation — Frederick’s syndrome.”
This occurs when complete AV block develops in the presence of ongoing atrial fibrillation. In such cases, the atria continue to fibrillate, while the ventricles are driven by an alternative pacemaker. However, the ventricular rate is typically low (around 30–40 bpm), so at higher heart rates, it is generally not necessary to consider Frederick’s syndrome.
Across these three examples, we have explored atrial fibrillation in detail. However, atrial fibrillation has a “relative” — not a twin, but a closely resembling rhythm — atrial flutter, and it is essential to learn how to differentiate between them. Let us now review atrial flutter, after which we will proceed to a practice task where atrial fibrillation and atrial flutter will be mixed together.