
LESSON 2 – Terminology and Fundamentals
From this point forward, we begin our formal training. We will start with a high-level overview of electrocardiography as a clinical tool.
Electrocardiography is the process of recording and analyzing the electrical activity generated by the heart. The primary output of this procedure is the electrocardiogram.
In simplified terms, as an electrical impulse propagates through the myocardium, it creates a wave of depolarization. This activity is captured by measuring action potentials via surface electrodes. The morphology of the resulting waveform is determined by several factors: the positioning of the active electrode, as well as the velocity and vector of the conduction wave.
Detailed electrophysiological processes are extensively documented in specialized literature; I encourage you to review those fundamentals. However, I am confident you have already covered this extensively during your medical training. Our objective here is to bypass dense electrophysiological theory and focus on the clinical essentials required for interpretation.
While you are undoubtedly familiar with the appearance of an ECG tracing, let’s perform a brief review of its primary components.
PICTURE – TYPICAL ECG
For standardization, ECGs are recorded on grid paper (millimeter paper). Each small square measures 1×1 mm, while each large block (heavy line) measures 5×5 mm. Most of the ECG presented in this course include automated interpretations and measurements calculated by the built-in program. They will serve as a helpful reference tool as you begin your training. While you may not always have access to these automated data points in a “real-world” clinical setting.
Paper Speed
Standard recording speeds are typically 25 mm/s or 50 mm/s (10 mm/s is rarely utilized). This setting is vital for calculating intervals and durations. At a paper speed of 50 mm/s, one small square corresponds to 0.02 s (20 ms). Conversely, at 25 mm/s, one small square represents 0.04 s (40 ms).
Voltage (Amplitude)
The standard gain is almost universally set at 10 mm = 1 millivolt (mV). Most ECG machines perform a calibration check before recording; the calibration spike (as shown in the illustration below) represents a 1 mV signal.
Leads
As you are aware, a standard ECG consists of 12 leads. While supplemental leads exist, they fall outside the scope of this course.
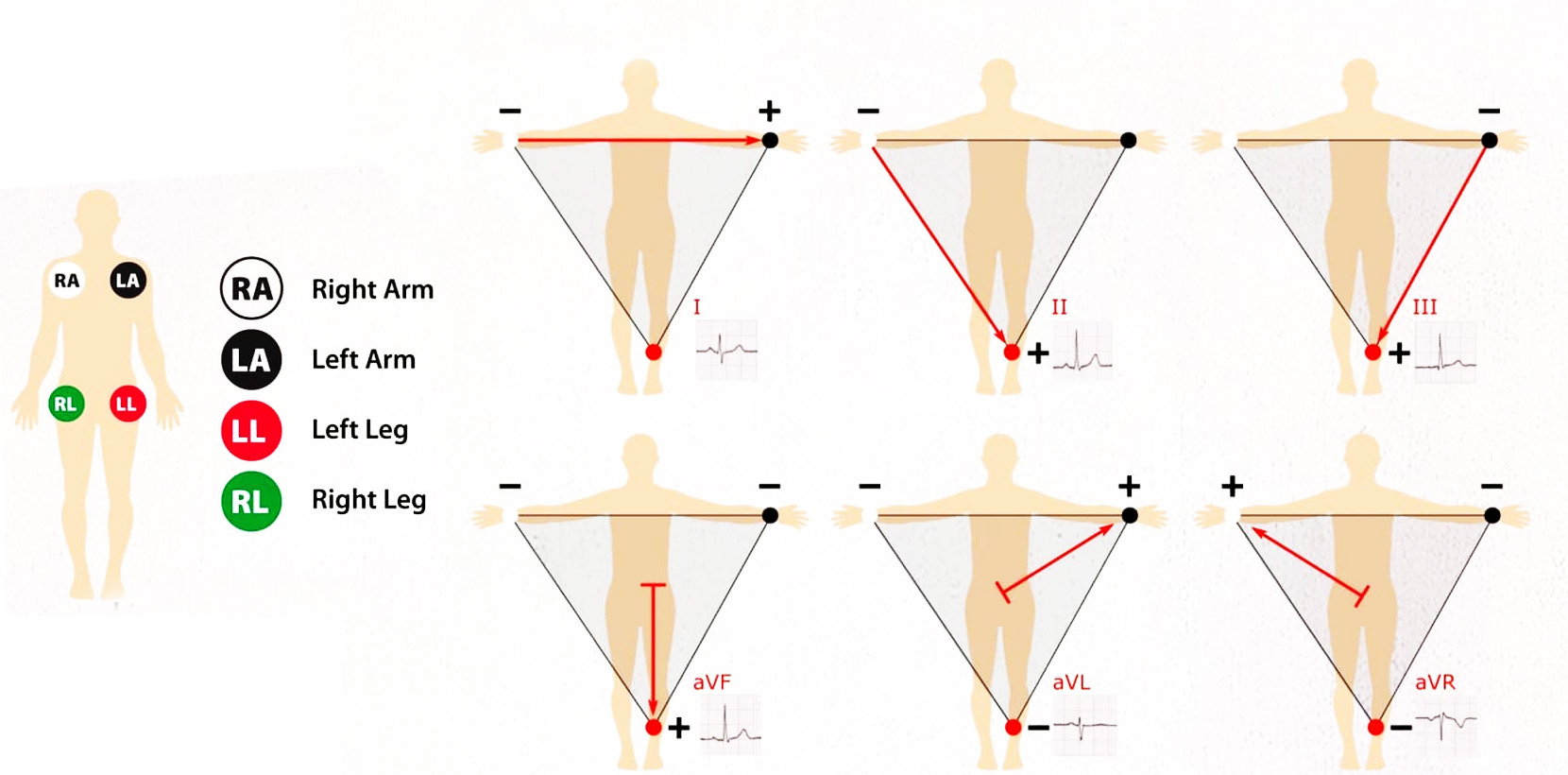
Limb Leads
Leads I, II, III, aVL, aVR, and aVF are classified as limb leads because the recording electrodes are placed on the patient’s extremities. Note that aVL is an augmented version of Lead I, and aVF is an augmented version of Lead III. For now, simply keep this relationship in mind.
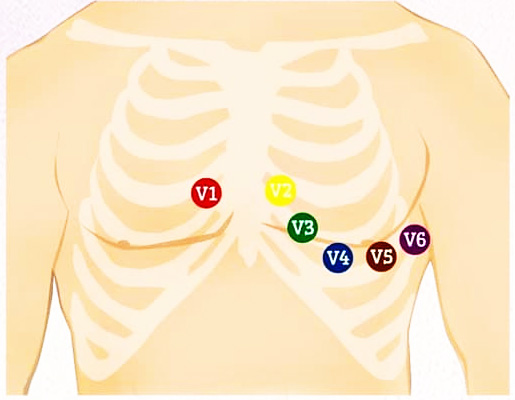
Precordial Leads
Leads V1 through V6 are known as precordial leads, with electrodes positioned across the chest wall. V1 and V2 are often referred to as the “right precordial leads,” while V5 and V6 are the “left precordial leads.” The anatomical basis for this nomenclature is evident in the illustration below.
Determining Heart Rate (HR)
Now that we have covered the fundamentals, we can proceed to one of the most basic tasks in ECG interpretation: calculating the heart rate.
This is a straightforward process. First, determine the duration of the RR interval, then choose one of the following methods. I recommend the following approach:
The Precise Method
- At a paper speed of 50 mm/s: HR = 3000 / RR (measured in mm).
- At a paper speed of 25 mm/s: HR = 1500 / RR (measured in mm)
The advantage of this method is its accuracy, especially with rapid tachyarrhythmias, though it may require a calculator.
The Simplified Method (The “Big Box” Method):
Clinicians often use a quicker estimation by counting the large squares (5 mm blocks):
At 50 mm/s: HR = 600 / number of large squares.
At 25 mm/s: HR = 300 / number of large squares.
Example Calculation:
Let’s calculate the heart rate using this ECG strip:
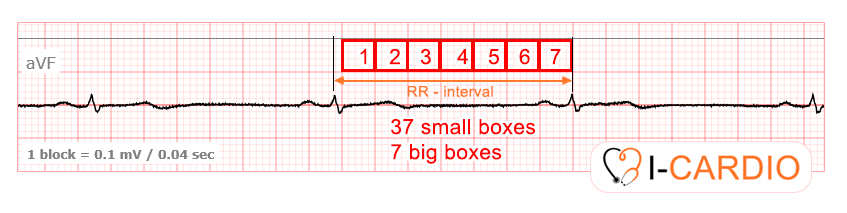
The paper speed is 25 mm/s (1 block = 0.04 sec). There are approximately 7 large squares within the RR interval.
- Simplified calculation: 300 / 7 ≈ 42 bpm.
- Precise calculation: Counting the small squares, the RR interval is 47 mm. Thus, 1500 / 37 ≈ 40 bpm. As you can see, the second method provides greater precision.
Clinical Note:
It is important to remember that RR intervals in consecutive cardiac cycles are rarely identical. Therefore, to determine the heart rate accurately, you should calculate the mean value of three or more consecutive RR intervals.
Please complete the following short exercise before we move forward.